General Information About Oropharyngeal Cancer
Oropharyngeal cancer is a type of head and neck cancer that starts in the tissues of the oropharynx.
The pharynx is a hollow tube in the neck about 5 inches long that is made up of three parts:
- The nasopharynx is the upper part of the pharynx, located behind the nose. The nostrils are connected to the nasopharynx. Openings on each side of the nasopharynx lead to the ears.
- The oropharynx is the middle part, located beneath the nasopharynx.
- The hypopharynx is the lowermost part of the pharynx, opening up to both the trachea (windpipe) and esophagus.
When we breathe or swallow, the pharynx acts as a passageway for air to reach the lungs and food to reach the stomach. Oropharyngeal cancer commonly begins in the squamous cells that line the oropharynx.
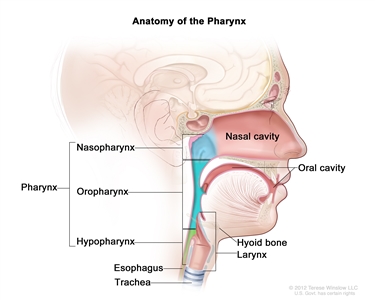
Anatomy of the pharynx. The pharynx is a hollow, muscular tube inside the neck that starts behind the nose and opens into the larynx and esophagus. The three parts of the pharynx are the nasopharynx, oropharynx, and hypopharynx.
The oropharynx includes the:
- soft palate
- side and back walls of the throat
- tonsils
- back one-third of the tongue
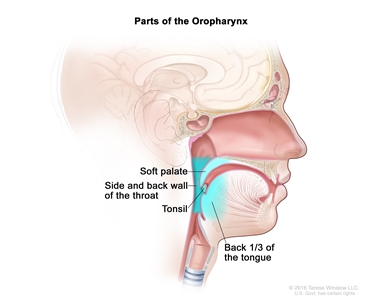
Parts of the oropharynx. The oropharynx includes the soft palate, the side and back walls of the throat, the tonsils, and the back one-third of the tongue.
Sometimes, a person can have more than one cancer at the same time in the oropharynx and mouth, nose, throat, voice box (larynx), windpipe (trachea), or esophagus.
Smoking or being infected with human papillomavirus (HPV) can increase the risk of oropharyngeal cancer.
Oropharyngeal cancer is caused by certain changes in how oropharyngeal cells function, especially how they grow and divide into new cells. There are many risk factors for oropharyngeal cancer, but many do not directly cause cancer. Instead, they increase the chance of DNA damage in cells that may lead to oropharyngeal cancer. Learn more about how cancer develops at What Is Cancer?
A risk factor is anything that increases a person's chance of getting a disease. Some risk factors for oropharyngeal cancer, like tobacco use, can be changed. Risk factors also include things you cannot change, like your family history. Learning about risk factors for oropharyngeal cancer can help you make choices that might prevent or lower your risk of getting it.
The most common risk factors for oropharyngeal cancer include:
- a history of smoking cigarettes for more than 10 pack years and other tobacco use
- heavy alcohol use
- being infected with human papillomavirus (HPV), especially HPV type 16
- a personal history of head and neck cancer
- chewing betel quid, a stimulant commonly used in parts of Asia
The number of cases of oropharyngeal cancers linked to HPV infection is increasing. Learn more about HPV and Cancer.
Signs and symptoms of oropharyngeal cancer include a lump in the neck and a sore throat.
Sometimes oropharyngeal cancer does not cause early signs and symptoms. When signs and symptoms occur, they may include:
- a sore throat that does not go away
- trouble swallowing
- trouble opening the mouth fully
- trouble moving the tongue
- weight loss for no known reason
- ear pain
- a lump in the back of the mouth, throat, or neck
- a white patch on the tongue or lining of the mouth that does not go away
- coughing up blood
These problems may be caused by conditions other than oropharyngeal cancer. Check with your doctor if you have any of these problems to find out the cause and begin treatment, if needed.
Tests that examine the mouth and throat are used to diagnose and stage oropharyngeal cancer.
If you have symptoms that suggest oropharyngeal cancer, your doctor will need to find out if these are due to cancer or another problem. They will ask when the symptoms started and how often you have been having them. They will also ask about your personal and family health history and do a physical exam. Based on these results, the doctor may recommend other tests. If you are diagnosed with oropharyngeal cancer, the results of these tests will help you and your doctor plan treatment.
The following tests and procedures are used to diagnose and stage oropharyngeal cancer:
- During a physical exam of the mouth and neck, the doctor or dentist looks at the mouth and neck, under the tongue, and down the throat with a small, long-handled mirror to check for abnormal areas.
- A neurological exam uses a series of questions and tests to check the brain, spinal cord, and nerve function. The exam checks your mental status, coordination, and ability to walk normally, and how well the muscles, senses, and reflexes work. This may also be called a neuro exam or a neurologic exam.
-
PET-CT scan combines the pictures from a positron emission tomography (PET) scan and a computed tomography (CT) scan. The PET and CT scans are done at the same time with the same machine. The combined scans give more detailed pictures of areas inside the body than either scan gives by itself.
- For the PET scan, a small amount of radioactive glucose (sugar) is injected into a vein. The scanner rotates around the body and makes a picture of where glucose is being used in the body. Because cancer cells often take up more glucose than normal cells, the pictures can be used to find cancer cells in the body.
- For the CT scan, a series of detailed pictures of areas inside the body, such as the head, neck, chest, and lymph nodes, is taken from different angles. A dye is injected into a vein or swallowed to help the organs or tissues show up more clearly.
-
MRI (magnetic resonance imaging) uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
-
Biopsy is the removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. A fine-needle biopsy is usually done to remove a sample of tissue using a thin needle.
The following procedures may be used to remove samples of cells or tissue:
- Endoscopy is a procedure to look at organs and tissues inside the body to check for abnormal areas. An endoscope is inserted through an incision (cut) in the skin or opening in the body, such as the mouth or nose. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove abnormal tissue or lymph node samples, which are checked under a microscope for signs of disease. The nose, throat, back of the tongue, esophagus, stomach, larynx, windpipe, and large airways will be checked. The type of endoscopy is named for the part of the body that is being examined. For example, pharyngoscopy is an exam to check the pharynx.
- Laryngoscopy is a procedure in which the doctor checks the larynx (voice box) with a mirror or a laryngoscope to check for abnormal areas. A laryngoscope is a thin, tube-like instrument with a light and a lens for viewing the inside of the throat and voice box. It may also have a tool to remove tissue samples, which are checked under a microscope for signs of cancer.
If cancer is found, the following test may be done to study the cancer cells:
- HPV test (human papillomavirus test) is a laboratory test used to check the sample of tissue for certain types of HPV infection, such as HPV type 16. This test is done because oropharyngeal cancer can be caused by HPV infection. This is important because HPV-positive oropharyngeal cancer has a better prognosis and is treated differently than HPV-negative oropharyngeal cancer.
Learn about the type of information that can be found in a pathologist's report about the cells or tissue removed during a biopsy at Pathology Reports.
Some people may decide to get a second opinion.
You may want to get a second opinion to confirm your oropharyngeal cancer diagnosis and treatment plan. If you seek a second opinion, you will need to get medical test results and reports from the first doctor to share with the second doctor. The second doctor will review the pathology report, slides, and scans. They may agree with the first doctor, suggest changes or another treatment approach, or provide more information about your cancer.
Learn more about choosing a doctor and getting a second opinion at Finding Cancer Care. You can contact NCI's Cancer Information Service via chat, email, or phone (both in English and Spanish) for help finding a doctor, hospital, or getting a second opinion. For questions you might want to ask at your appointments, visit Questions to Ask Your Doctor About Cancer.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis depends on:
- whether the person has HPV infection of the oropharynx
- whether the person has a history of smoking cigarettes for 10 or more pack years
- the stage of the cancer
- the number and size of lymph nodes with cancer
Oropharyngeal tumors related to HPV infection have a better prognosis and are less likely to recur than tumors not linked to HPV infection.
Treatment options depend on:
- the stage of the cancer
- keeping the person's ability to speak and swallow as normal as possible
- the person's general health
People with oropharyngeal cancer have an increased risk of another cancer in the head or neck. This risk is increased if a person continues to smoke or drink alcohol after treatment.
For more information, visit Cigarette Smoking: Health Risks and How to Quit.
Stages of Oropharyngeal Cancer
Cancer stage describes the extent of cancer in the body.
Cancer stage describes the extent of cancer in the body, such as the size of the tumor, whether it has spread, and how far it has spread from where it first formed. Knowing the cancer stage helps plan treatment.
There are several staging systems for cancer that describe the extent of the cancer. Oropharyngeal cancer staging usually uses the TNM staging system. The cancer may be described by this staging system in your pathology report. Based on the TNM results, a stage (I, II, III, or IV, also written as 1, 2, 3, or 4) is assigned to the cancer. When talking to you about your diagnosis, your doctor may describe the cancer as one of these stages.
Learn more about Cancer Staging.
The following stages are used for HPV-positive oropharyngeal cancer:
Stage I (also called stage 1) oropharyngeal cancer
In stage I, one of the following is true:
- one or more lymph nodes with cancer that is HPV 16–positive are found but the place where the cancer began is not known. The lymph nodes with cancer are 6 centimeters or smaller, on one side of the neck; or
- cancer is found in the oropharynx (throat) and the tumor is 4 centimeters or smaller. Cancer may have spread to one or more lymph nodes that are 6 centimeters or smaller, on the same side of the neck as the primary tumor.
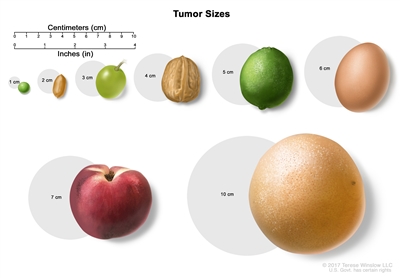
Tumor sizes are often measured in centimeters (cm) or inches. Common food items that can be used to show tumor size in cm include: a pea (1 cm), a peanut (2 cm), a grape (3 cm), a walnut (4 cm), a lime (5 cm or 2 inches), an egg (6 cm), a peach (7 cm), and a grapefruit (10 cm or 4 inches).
Stage II (also called stage 2) oropharyngeal cancer
In stage II, one of the following is true:
- one or more lymph nodes with cancer that is HPV 16–positive are found but the place where the cancer began is not known. The lymph nodes with cancer are 6 centimeters or smaller, on one or both sides of the neck; or
- the tumor is 4 centimeters or smaller. Cancer has spread to lymph nodes that are 6 centimeters or smaller, on the opposite side of the neck as the primary tumor or on both sides of the neck; or
- the tumor is larger than 4 centimeters or cancer has spread to the top of the epiglottis (the flap that covers the trachea during swallowing). Cancer may have spread to one or more lymph nodes that are 6 centimeters or smaller, anywhere in the neck.
Stage III (also called stage 3) oropharyngeal cancer
In stage III, one of the following is true:
- cancer has spread to the larynx (voice box), front part of the roof of the mouth, lower jaw, muscles that move the tongue, or to other parts of the head or neck. Cancer may have spread to lymph nodes in the neck; or
- the tumor is any size and cancer may have spread to the larynx, front part of the roof of the mouth, lower jaw, muscles that move the tongue, or to other parts of the head or neck. Cancer has spread to one or more lymph nodes that are larger than 6 centimeters, anywhere in the neck.
Stage IV (also called stage 4) oropharyngeal cancer
In stage IV, cancer has spread to other parts of the body, such as the lung or bone.
Stage IV oropharyngeal cancer is also called metastatic oropharyngeal cancer. Metastatic cancer happens when cancer cells travel through the lymphatic system or blood and form tumors in other parts of the body. The metastatic tumor is the same type of cancer as the primary tumor. For example, if oropharyngeal cancer spreads to the lung, the cancer cells in the lung are actually oropharyngeal cancer cells. The disease is called metastatic oropharyngeal cancer, not lung cancer. Learn more in Metastatic Cancer: When Cancer Spreads.
The following stages are used for HPV-negative oropharyngeal cancer:
Stage 0 (also called carcinoma in situ of the oropharynx)
In stage 0, abnormal cells are found in the lining of the oropharynx (throat). These abnormal cells may become cancer and spread into nearby normal tissue.
Stage I (also called stage 1) oropharyngeal cancer
In stage I, cancer has formed. The tumor is 2 centimeters or smaller.
Tumor sizes are often measured in centimeters (cm) or inches. Common food items that can be used to show tumor size in cm include: a pea (1 cm), a peanut (2 cm), a grape (3 cm), a walnut (4 cm), a lime (5 cm or 2 inches), an egg (6 cm), a peach (7 cm), and a grapefruit (10 cm or 4 inches).
Stage II (also called stage 2) oropharyngeal cancer
In stage II, the tumor is larger than 2 centimeters but not larger than 4 centimeters.
Stage III (also called stage 3) oropharyngeal cancer
In stage III, the cancer:
- is either larger than 4 centimeters or has spread to the top of the epiglottis (the flap that covers the trachea during swallowing); or
- is any size. Cancer has spread to one lymph node that is 3 centimeters or smaller, on the same side of the neck as the primary tumor.
Stage IV (also called stage 4) oropharyngeal cancer
Stage IV is divided into stages IVA, IVB, and IVC.
- In stage IVA, cancer:
- has spread to the larynx (voice box), front part of the roof of the mouth, lower jaw, or muscles that move the tongue. Cancer may have spread to one lymph node that is 3 centimeters or smaller, on the same side of the neck as the primary tumor; or
- is any size and may have spread to the top of the epiglottis, larynx, front part of the roof of the mouth, lower jaw, or muscles that move the tongue. Cancer has spread to one of the following:
- one lymph node that is larger than 3 centimeters but not larger than 6 centimeters, on the same side of the neck as the primary tumor; or
- more than one lymph node that is 6 centimeters or smaller, anywhere in the neck.
- In stage IVB, cancer:
- has spread to the muscle that moves the lower jaw, the bone attached to the muscle that moves the lower jaw, the base of the skull, or to the area behind the nose or around the carotid artery. Cancer may have spread to lymph nodes in the neck; or
- may be any size and may have spread to other parts of the head or neck. Cancer has spread to a lymph node that is larger than 6 centimeters or has spread through the outside covering of a lymph node into nearby connective tissue.
- In stage IVC, cancer has spread to other parts of the body, such as the lung, liver, or bone.
Stage IV oropharyngeal cancer is also called metastatic oropharyngeal cancer. Metastatic cancer happens when cancer cells travel through the lymphatic system or blood and form tumors in other parts of the body. The metastatic tumor is the same type of cancer as the primary tumor. For example, if oropharyngeal cancer spreads to the lung, the cancer cells in the lung are actually oropharyngeal cancer cells. The disease is called metastatic oropharyngeal cancer, not lung cancer. Learn more in Metastatic Cancer: When Cancer Spreads.
Oropharyngeal cancer can recur (come back) after it has been treated.
Recurrent oropharyngeal cancer is cancer that has come back after it has been treated. If oropharyngeal cancer comes back, it may come back in the oropharynx, lymph nodes, or other parts of the body, such as the lungs, bone, or liver. Tests will help determine where in the body the cancer has returned. The type of treatment that you have for recurrent oropharyngeal cancer will depend on where it has come back.
Learn more in Recurrent Cancer: When Cancer Comes Back. Information to help you cope and talk with your health care team can be found in the booklet When Cancer Returns.
Treatment Option Overview
There are different types of treatment for people with oropharyngeal cancer.
Different types of treatments are available for oropharyngeal cancer. You and your cancer care team will work together to decide your treatment plan, which may include more than one type of treatment. Many factors will be considered, such as the stage of the cancer, your overall health, and your preferences. Your plan will include information about your cancer, the goals of treatment, your treatment options and the possible side effects, and the expected length of treatment.
Talking with your cancer care team before treatment begins about what to expect will be helpful. You'll want to learn what you need to do before treatment begins, how you'll feel while going through it, and what kind of help you will need. Learn more at Questions to Ask Your Doctor About Your Treatment.
People with oropharyngeal cancer should have their treatment planned by a team of doctors with expertise in treating head and neck cancer.
An oncologist, a doctor who specializes in treating people with cancer, oversees treatment for oropharyngeal cancer. Because the oropharynx helps in breathing, eating, and talking, you may need help adjusting to the side effects of the cancer and its treatment. The oncologist may refer you to other health care providers who are experts in treating head and neck cancer and also specialize in other areas of medicine. Other specialists may include:
- head and neck surgeon
- radiation oncologist
- plastic surgeon
- dentist
- dietitian
- psychologist
- rehabilitation specialist
- speech therapist
The following types of treatment are used:
Surgery
Surgery to remove the tumor is a common treatment for all stages of oropharyngeal cancer. A surgeon may remove the cancer and some of the healthy tissue around the cancer. After the surgeon removes all the cancer that can be seen at the time of the surgery, some people may be given chemotherapy or radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
New types of surgery, including transoral robotic surgery, are being studied for the treatment of oropharyngeal cancer. Transoral robotic surgery may be used to remove cancer from hard-to-reach areas of the mouth and throat. Cameras attached to a robot give a 3-dimensional (3D) image that a surgeon can see. Using a computer, the surgeon guides very small tools at the ends of the robot arms to remove the cancer. This procedure may also be done using an endoscope.
Learn more about Surgery to Treat Cancer.
Radiation therapy
Radiation therapy uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing by damaging their DNA. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer.
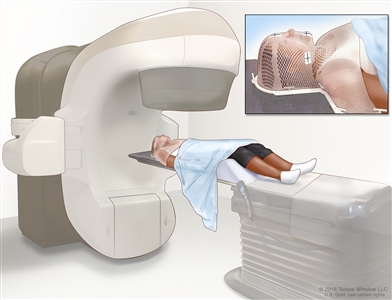
External-beam radiation therapy of the head and neck. A machine is used to aim high-energy radiation at the cancer. The machine can rotate around the patient, delivering radiation from many different angles to provide highly conformal treatment. A mesh mask helps keep the patient's head and neck from moving during treatment. Small ink marks are put on the mask. The ink marks are used to line up the radiation machine in the same position before each treatment.
Certain ways of giving radiation therapy can help keep radiation from damaging nearby healthy tissue. These types of radiation therapy include:
- Intensity-modulated radiation therapy (IMRT): IMRT is a type of 3-dimensional (3-D) radiation therapy that uses a computer to make pictures of the size and shape of the tumor. Thin beams of radiation of different intensities (strengths) are aimed at the tumor from many angles.
- Stereotactic body radiation therapy: Stereotactic body radiation therapy is a type of external radiation therapy. Special equipment is used to place the person in the same position for each radiation treatment. Once a day for several days, a radiation machine aims a larger than usual dose of radiation directly at the tumor. By having the person in the same position for each treatment, there is less damage to nearby healthy tissue. This procedure is also called stereotactic external-beam radiation therapy and stereotaxic radiation therapy.
In advanced oropharyngeal cancer, dividing the daily dose of radiation into smaller-dose treatments improves the way the tumor responds to treatment. This is called hyperfractionated radiation therapy.
Radiation therapy may work better in people who have stopped smoking before beginning treatment.
If the thyroid or pituitary gland are part of the radiation treatment area, the person has an increased risk of hypothyroidism (too little thyroid hormone). A blood test to check the thyroid hormone level in the body should be done before and after treatment.
Chemotherapy
Chemotherapy uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. Chemotherapy for oropharyngeal cancer is usually systemic, meaning it is taken by mouth or injected into a vein or muscle. When given this way, the drugs enter the bloodstream and can reach cancer cells throughout the body.
Chemotherapy drugs used to treat oropharyngeal cancer include:
- cisplatin
- docetaxel
- fluorouracil
- paclitaxel
Combinations of these drugs may be used. Other chemotherapy drugs not listed here may also be used.
Chemotherapy may be combined with other types of treatment, such as radiation therapy.
To learn more about how chemotherapy works, how it is given, common side effects, and more, visit Chemotherapy to Treat Cancer and Chemotherapy and You: Support for People With Cancer.
Targeted therapy
Targeted therapy uses drugs or other substances to identify and attack specific cancer cells. Cetuximab is a type of targeted therapy used to treat recurrent and metastatic oropharyngeal cancer.
Learn more about Targeted Therapy to Treat Cancer.
Immunotherapy
Immunotherapy is a treatment that uses a person's immune system to fight cancer. Your doctor may suggest biomarker tests to help predict your response to certain immunotherapy drugs. Learn more about Biomarker Testing for Cancer Treatment.
Pembrolizumab and nivolumab are types of immunotherapy used to treat metastatic or recurrent oropharyngeal cancer.
Learn more about Immunotherapy to Treat Cancer.
New types of treatment are being tested in clinical trials.
A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. For some patients, taking part in a clinical trial may be an option.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
To learn more about clinical trials, see Clinical Trials Information for Patients and Caregivers.
Treatment for oropharyngeal cancer may cause side effects.
For information about side effects caused by treatment for cancer, visit our Side Effects page.
Follow-up care may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
After treatment is complete, it is important to have head and neck exams to look for signs that the cancer has come back. Check-ups will be done every 6 to 12 weeks in the first year, every 3 months in the second year, every 3 to 4 months in the third year, and every 6 months thereafter.
Treatment of Stage I and Stage II Oropharyngeal Cancer
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of newly diagnosed stage I and stage II oropharyngeal cancer may include:
- radiation therapy
- surgery
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Stage III and Nonmetastatic Stage IV Oropharyngeal Cancer
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of newly diagnosed stage III oropharyngeal cancer and stage IV oropharyngeal cancer may include:
- radiation therapy with or without chemotherapy given at the same time, for people with locally advanced cancer
- radiation therapy alone for people who cannot have chemotherapy
- chemotherapy given at the same time as radiation therapy
- chemotherapy followed by radiation therapy given at the same time as more chemotherapy
- a clinical trial of immunotherapy (nivolumab) with chemotherapy given at the same time as radiation therapy in people with cancer that has a higher risk of coming back
- a clinical trial of radiation therapy with or without chemotherapy
- a clinical trial of transoral surgery followed by standard- or low-dose radiation therapy with or without chemotherapy in people with HPV-positive oropharyngeal cancer
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Metastatic Stage IV and Recurrent Oropharyngeal Cancer
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of oropharyngeal cancer that has metastasized or recurred in the oropharynx may include:
- surgery, if the cancer does not respond to radiation therapy
- radiation therapy, if the tumor was not completely removed by surgery and previous radiation has not been given
- second surgery, if the tumor was not completely removed by the first surgery
- chemotherapy for people with recurrent cancer that cannot be removed by surgery
- radiation therapy given at the same time as chemotherapy
- stereotactic body radiation therapy given at the same time as targeted therapy (cetuximab)
- immunotherapy (nivolumab or pembrolizumab) given after or during chemotherapy
- clinical trials of targeted therapy, stereotactic body radiation therapy, hyperfractionated radiation therapy, or immunotherapy given at the same time as chemotherapy
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
To Learn More About Oropharyngeal Cancer
For more information from the National Cancer Institute about oropharyngeal cancer, visit:
For general cancer information and other resources from the National Cancer Institute, visit:
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute's (NCI's) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government's center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of oropharyngeal cancer. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary ("Updated") is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become "standard." Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI's website. For more information, call the Cancer Information Service (CIS), NCI's contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as "NCI's PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary]."
The best way to cite this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Oropharyngeal Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/head-and-neck/patient/adult/oropharyngeal-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389310]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website's E-mail Us.
Last Revised: 2024-04-26
If you want to know more about cancer and how it is treated, or if you wish to know about clinical trials for your type of cancer, you can call the NCI's Cancer Information Service at 1-800-422-6237, toll free. A trained information specialist can talk with you and answer your questions.